
Research Article | DOI: https://doi.org/10.31579/2578-8868/008
1 Neurosurgery Department, Mansoura University
*Corresponding Author: Ahmed Zaher, Neurosurgery Department, Mansoura University.
Citation: Ahmed Zaher, Microsurgical Excision of Herniated Lumber Disc in Pediatric Population, J Neuroscience and Neurological Surgery. Doi: 10.31579/2578-8868/008
Copyright: © 2018 Ahmed Zaher. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 30 May 2018 | Accepted: 15 June 2018 | Published: 25 June 2018
Keywords: nuerological disorders;nuerological degenerative diseases
Introduction: Lumbar disc herniation is a relatively rare disorder among children and adolescent population compared to adults. The objectives of this work are to study the lumbar disc herniation in pediatric population and determine the surgical outcome of lumbar microdiscectomy in such population. Patients and methods: A series of 32 pediatric patients less than 18 years operated by microdiscectomy at Mansoura University hospital during the period from January 2005 to March 2015 were retrospectively analyzed. Clinical presentation, physical signs, predisposing factors, radiological investigations and operative findings were retrieved from medical records. Improvement of pain was assessed by visual analogue scale. Results: The study included 17 females (53.1%) and 15 males (46.9%) ranging in age from 10 to18 years (mean, 14.2 year). The patients were followed up for periods ranging from three to 115 months (mean, 55 months). All patients had radicular pain (100%) with additional back pain in twenty one patients (65.63%), twenty eight patients (87.5%) presented by sciatic pain while six patients (18.75%) showed femoral neuralgia. Straight leg raising test was positive in 90.62%. L4/5 was the commonest affected level in eighteen patients (56.25%) while twelve patients (37.5%) had disc herniation at L5-S1 level and only two patients had herniation at L3-4 disc level. Family history of lumbar disc herniation in first degree relative was positive in twenty one patients (65.63%). History of relevant trauma was documented in only twelve patients (37.5%). During surgery the disc was soft, rubbery and well hydrated in 90.6% of cases. Subligamentous disc herniation was observed in 81%, while 12.5% of patients had disc bulge with intact annulus and only 6.5% had extruded disc. All patients showed significant improvement of radicular pain at the time of discharge while back pain continued to improve during early postoperative follow up. Low back pain and radicular pain equally improved after three months despite instant postoperative improvement of radicular pain. Postoperative complications were rare and included one case of wound infection, one case of iatrogenic CSF leak and new neurological deficit in another case. Conclusion: Lumbar disc herniation in pediatric population differs from that of adults in many aspects. Microdiscectomy is safe and reliable procedure for management of pediatric lumbar disc herniation with good outcome and minimal morbidity
Lumbar disc herniation (LDH) is well known degenerative disorder of human spine with high prevalence among adults as a result of degenerative process. LDH in pediatrics is a relatively uncommon disease which accounts approximately for 0.5-5% of all patients undergoing surgery for lumbar disc herniation 1.
Several predisposing factors have been implicated: genetic and familial, trauma, growth spurts, elevated body mass index, epiphyseal ring separation, nutritional factors and vertebral anomalies such as transitional vertebra6,7.
The incidence of symptomatic pediatrics and adolescents with LDH range between 0.5%- 6.8% of all LDH cases2,3,8,9. Clinical presentation of LDH in pediatrics is similar to that of adults including low back pain, radicular pain (sciatica or femoral neuralgia), sensory and motor deficits and diminished reflexes. Nerve root stretch signs like straight leg raising test or femoral stretch test are distinctive in pediatric patients more than adults because pediatrics' nerve roots are under greater tension than adults, a finding that also explains the relative risk of post operative radicular deficit after vigorous surgical manipulation of over stretched roots. 3
Because the immature growing pediatric spine is liable for undesirable surgical trauma with postoperative iatrogenic deformity, a trial of conservative management for 1-3 months should be the first treatment option in neurologically intact patients 3,5,11 Despite the pediatric LDH patients do not respond well to conservative treatment as adults 10,11.
The first operation of lumbar discectomy in pediatrics had been done by Wahren in 1945 to remove a disc of twelve years old child, 12 since then discectomy for pediatrics is not an uncommon procedure. Surgical indications for LDH in pediatrics are similar to those of adults which include cauda equine syndrome, progressive motor weakness and intractable pain with failed adequate conservative management and associated spinal deformities or congenital anomalies 3,13,14.
Surgical procedures for treatment of LDH in pediatrics are similar to adults and include traditional laminectomy, hemilaminectomy, laminotomy and discectomy, percutaneous endoscopic discectomy, microdiscectomy and spinal fusion. 3, 15
In this retrospective study, we aim to evaluate the efficacy of microdiscectomy in management of lumbar disc prolapse among pediatric patients and to discuss the distinctive features of lumbar disc herniation in this age group.
This is a series of consecutive thirty two pediatric patients (less than 18 years old), 17 females and 15 males with mean age of 14.2 years (range, 10 to 18 years) with symptomatic lumbar disc herniation operated by microdiscectomy at Mansoura University Hospital between January 2005 to March 2015. Thirty two pediatric patients who fulfilled the inclusion criteria were enrolled in this study.
Our study included patients less than 18 years old with unilateral leg pain, with or without LBP after failure of conservative treatment with unilateral lumbar disc herniation and operated by microdiscectomy. Our exclusion criteria included patients with cauda equine syndrome, prior lumbar surgery, disc space infection, spinal fracture, spinal tumor, spinal stenosis or spondylolithesis.
All patients were complaining of leg pain with or without back pain and all received trials of conservative management with no adequate response. MRI lumbosacral spine and X-ray in both posterior anterior and lateral extension flexion views were done for all patients before operation. The patients' files were reviewed as regards history, full neurological examination and postoperative outcome. Pain was scored using visual analogue scale (VAS) for both back and leg pain preoperatively, at time of discharge, one month and 3 months postoperatively. Operative details and follow up notes including neurological status were also reviewed.
Surgical approaches:
Patients were operated in the prone position with their head turned to one side, under general anesthesia. All patients were given single prophylactic dose of 50 mg/Kg Ampicillin-Sulbactam antibiotic The desired level was identified and confirmed under fluoroscopy. Through a small (4 cm) midline skin incision paraspinal muscles were striped in subperiosteal fashion under microscopic magnification to expose the interlaminal space on one side. A fenestration in ligamentum flavum had been sharply done starting laterally. Usually we face the epidural fat covering nerve root but in some cases with ruptured disc and sequestrated fragment the anteriorly compressed nerve root lies directly under the ligament. We faced a sequestrated fragment posterior to nerve root in one case. Following the identification of nerve root it was gently manipulated to expose the herniated disc anteriorly. Incision of posterior annulus was made and the disc tissues were removed by different shape punches and forceps till all detached nucleus was removed. A radical excision of the disc involving curettage of the disc space were not employed. A blunt hook was advanced to check any sequestrated subligamentous fragment. Then the wound was irrigated and fascial, deep dermal, and subcuticular layers were closed using absorbable sutures.
The study included seventeen females (53.1%) and fifteen males (46.9%). The age ranged from 10 to18 years (mean, 14.2 year). Table 2 shows the distribution of gender and mean age according to the herniated level. The patients were followed up for periods ranging from 3 to 115 months (mean 55 months). All patients had radicular pain (100%), while twenty one patients (65.6%) had back pain. Twenty six patients (81.2%) presented by sciatic pain while six patients (18.8%) (Two patients with L3-4 disc and four patients with L4-5 disc) showed femoral neuralgia, (Table 2)
Preoperative neurological examination revealed sensory changes in twenty three patients (71.9%), motor deficit in fourteen patients (43.8%) while nerve root stretch tests were positive in twenty nine patients (90.6%). L4/5 was the commonest affected level in eighteen patients (56.3%) while twelve patients (37.5%) had disc herniation at L5-S1 level and only two patients had herniation at L2-4 level. Family history of lumbar disc herniation in first degree relative was positive in twenty one patients (65.6%) of the cases while history of significant trauma was documented in only twelve patients (37.5%) (Table 2)
Ten patients (31.3%) had persistent motor weakness at time of discharge with only three patients (9.4%) continued to experience motor deficit after one month and all of them improved after three months follow up visits. Four patients out of twenty three patients complaining of sensory deficits improved as the time discharge, whereas fourteen patients (43.8%) continued to complain of sensory deficits after one month and only five patients (15.6%) had persistent sensory deficits at three months follow up (table 1).
During surgery the disc was soft, rubbery and well hydrated in 29 patients (90.6% of cases). Subligamentous disc herniation was observed in 81%, while 12.5% of patients had disc bulge with intact annulus and only 6.5% had extruded disc (fig. 1).
All patients showed significant improvement of VAS on discharge 1.62+0.83 for radicular pain (average+ standard deviation) and 2.35+0.75 for back pain and in comparison with preoperative 8.65+1.35 and 6.10+1.22 respectively and this improvement continued on first month to be 0.95+0.75 for radicular pain and 1.25+0.35 for back pain and after 3 months 0.65+0.53 and 0.35+0.24 for radicular and back pain respectively (table 1).
Postoperative complications were minimal and included one case of superficial wound infection that was managed conservatively by repeated wound dressing and intravenous antibiotic, one case of unintended durotomy which was repaired intraoperatively. Another case of L4-5 disc showed post operative new motor deficit that has been improved after three months on physiotherapy (table 3).
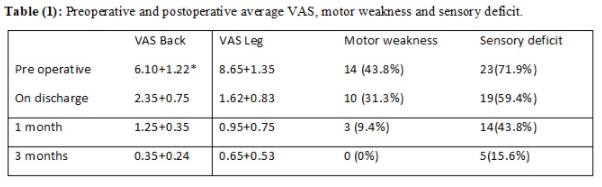
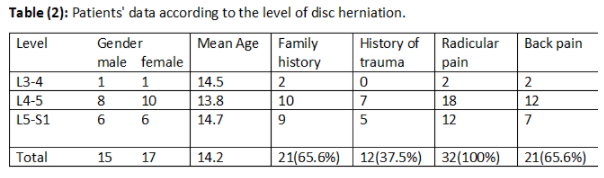
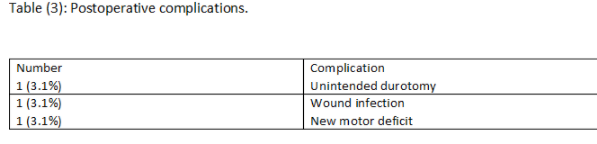
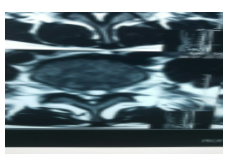
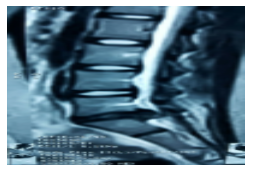
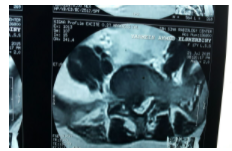
Fig. (1) a-d: Preoperative MRI of two of our cases: a, b Sagittal and axial MRI of the first case showing herniation of a well hydrated nuclus, c, d Sagittal and axial MRI of the second case showing L5-S1 disc with foraminal herniation.
Lumbar disc herniation not only affects adults but children and adolescents are also affected as well. LDH in pediatrics shares many aspects with those of adults while some physiological features of children and adolescents contradict adult LDH in various distinctive features. However, almost all attention was given to adult LDH while pediatric LDH remained partially understood 3.
History of significant trauma before the onset of symptoms was considered as a potential predisposing cause of lumbar disc herniation in children. 30–60% incidence of trauma had been reported in the literatures dissimilar to adult patients who usually do not have traumatic experiences before their symptoms 3,4,5. We found the same finding as twelve of our patients (37.5%) gave history of significant trauma preceding their pain. Some authors considered trauma as an etiology and others suggest that trauma is likely to be an inciting event in the exacerbation of the pre-existing disc lesions like micro-damage and degenerative changes instead of being a primary contributory factor 5,16. Another distinctive feature of pediatric population is strong family history; we found twenty one patients (65.63%) with a family history of lumbar disc herniation in their first degree relatives. Previous studies reported that 13 to 57% of children and adolescents with LDH had a first-degree relative with the same disorder 3,4,11.
The female predominance in our patients was supported by other studies 2,9,10,11,17. Çelik explained this gender preponderance by earlier bony and ligamentous maturation of girls compared to boys 17.
The clinical presentation of LDH in pediatrics is similar to that of adults either in presenting symptoms or affected levels. The majority of our cases had L4-5 (56.25%) and L5-S1 (37.5%) levels, moreover back pain and radiculopathy were the main presenting symptoms while it differs from adults in some findings as we found a higher ratio of nerve roots stretch tests (90.6% in our patients) between 30-60º compared to adults as consistent with other series 2,3,9,11. This could be explained by a higher nerve root tension for pediatric patients than that of adult patients. This finding as well as the lack of degenerative process in pediatrics explain the higher ratio of radicular pain compared to back pain 18.
It has been widely agreed by most reports that conservative treatment is not as effective for pediatric LDH as for that in adults 3,4,5,15. This finding gave explanation to the short periods of conservative treatment (4-6weeks) in neurologically intact patients in our series. Some authors provide three months of the conservative trials while others advocate a brief conservative periods even for neurologically intact patients with persistent disabling pain based on the previous agreement 2,4,9,19.
Poor response to conservative treatment in pediatrics is attributed to many factors like the viscosity and high elasticity of the intervertebral disc in children compared with that in adults19. Moreover pediatrics are more active and not complying well to the rest with a higher incidence of annular tear and epiphyseal cartilaginous disruption with a creation of a hard compressing fragment 20.
The previous findings also clear out our results of soft rubbery consistency of excised discs (90.6%) which also were resilient to be fully evacuated. We didn't use any aggressive curettage for disc removal to avoid disruption of a partially fused epiphyseal cartilage.
Discectomy remains the mostly used surgical procedure for LDH in children and adolescents as well as in adults. It is generally agreed in the literature that posterior discectomy with partial laminotomy is indicated for posterolateral disc herniation, whereas hemilaminotomy or laminectomy is required in cases of central disc herniation associated with spinal stenosis.3 In this study we included only cases with posterolateral herniation, while those who required decompressive procedures or fusion were excluded. Our techniques minimized the trauma to the pediatric growing spine preserving the ligamentum flavum, muscle, lamina, and facet joints in order to minimize iatrogenic instability and post operative epidural scar.
The overall improvement of leg pain was greater than that achieved in back pain which was demonstrated by better improvement of VAS, a finding that was clearly pronounced at early post operative period and this residual back pain can be explained by pain provocation from surgical incision, muscle dissection and ligamentous opening. Dewing et al. reported the same finding on his report of 197 young adult patients. 21
At three months follow up, the VAS for both leg pain and back pain were nearly equal which is different than adult patients who continue to demonstrate residual back pain.22his finding may be explained by the lack of associated degenerative process which continue to be a pain progenitor in adult spine. Another explanation is the lack of legalization and seek for compensation in this age group as well as lower incidence of psychiatric co morbidities in pediatrics compared to adults 17.
Motor weakness was improved in all patients (100%) while sensory deficit was improved in twenty-seven patients (84.4%). This good outcome with negligible complication rate are comparable to other studies that reported the outcome of microdiscectomy in adults21,23 and pediatrics 11,15,24,25,26,27.
Conclusion:
Microdiscectomy seems to be an effective, safe, simple and minimally invasive procedure for relief of radicular and back pain due to lumbar disc herniation in pediatrics. Nevertheless a longer follow-up period and a larger number of patients are needed to assess the long-term efficacy of this procedure.
Conflict of Interest/ Disclosures:
The author declare that they have no financial or other conflicts of interest in relation to this research and its publication.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
